


A Look at Biphasic Anaphylaxis
In this cohort, all instances occurred within four hours.
It’s always useful to describe the outcomes of patients treated with anaphylaxis. The life-threatening nature of the presentation and reliable treatment pathway limits the appetite for much randomized evaluation in this space, so using observational data to reinforce safe practice remains important.
This is just a single-center summary of pediatric patients treated over a seven year period at the Mt. Sinai emergency departments. Table 2 tells you everything they were able to dredge out of Epic:
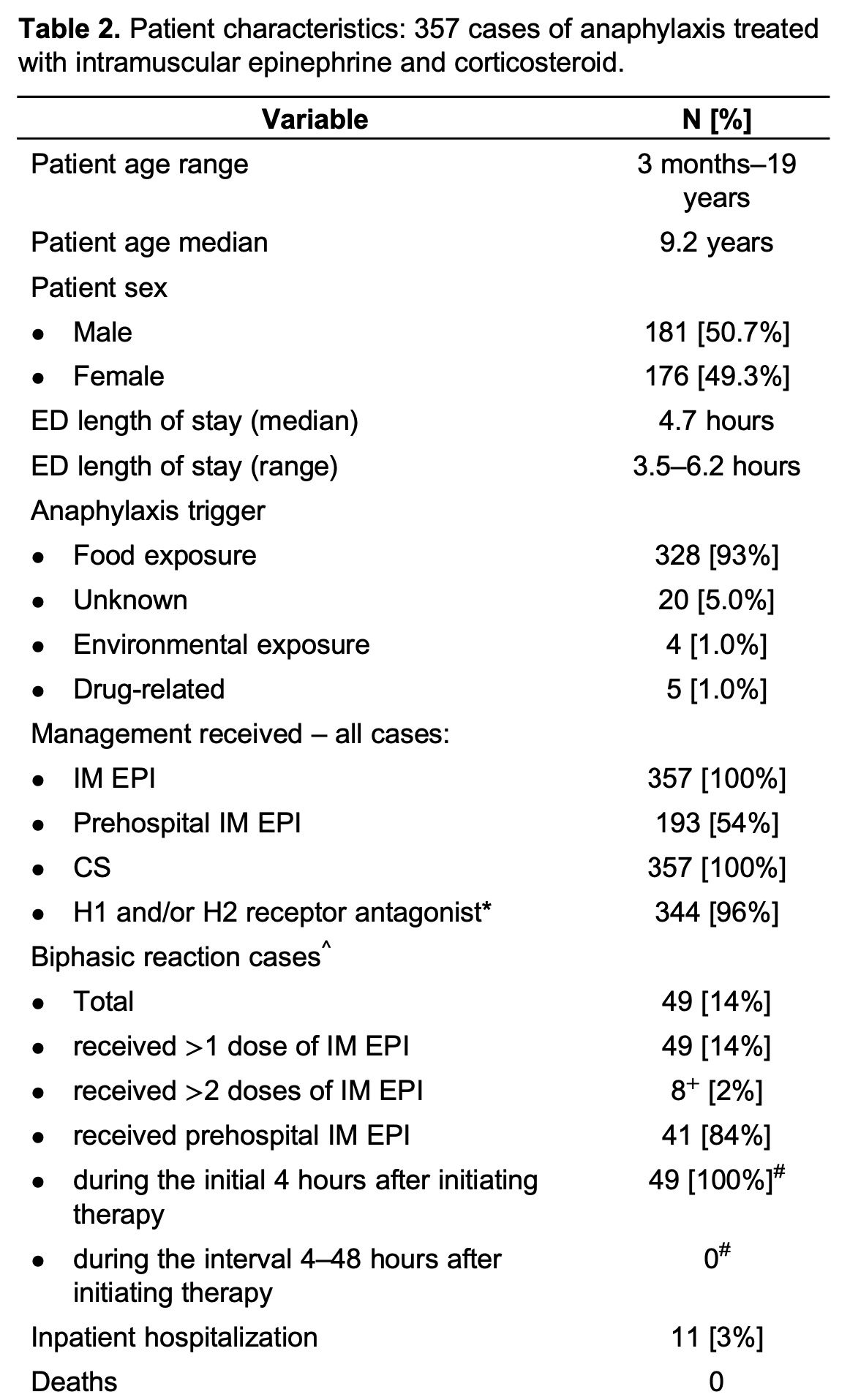
Obviously, everyone received intramuscular epinephrine (adrenaline). More unusual, everyone received corticosteroids, and nearly all received an H1 or H2 antagonist. Amusingly, they pat themselves on the back for this, despite citing several guidelines and analyses suggesting corticosteroids have no role due to lack of efficacy.
The primary useful takeaway in this instance is simply to toss their rates of biphasic reactions into the evidence pool. Specifically, the bit where all biphasic reactions occurred within 4 hours adds reassurance to practice patterns incorporating that general timeframe into observation. The authors chalk up their lack of biphasic reactions between 4-48 hours to their epinephrine + steroids + antihistamine institutional protocol – but, they would only be able capture symptom recurrence if the child returned to one of their three included EDs, or if subsequent documentation happened to mention the same.
So, still, epinephrine is all you really need for anaphylaxis. Antihistamines can be useful as needed for symptomatic pruritis, but corticosteroids are of unproven value.